Stab Wound Pathophysiology 622x4n
This document was ed by and they confirmed that they have the permission to share it. If you are author or own the copyright of this book, please report to us by using this report form. Report r6l17
Overview 4q3b3c
& View Stab Wound Pathophysiology as PDF for free.
More details 26j3b
- Words: 1,201
- Pages: 5
PATHOPHYSIOLOGY STAB INJURY
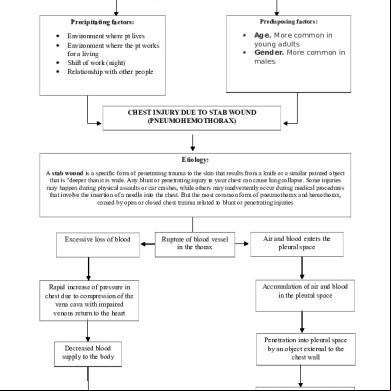
Predisposing factors:
Precipitating factors:
Environment where pt lives Environment where the pt works for a living Shift of work (night) Relationship with other people
Age. More common in young adults Gender. More common in males
CHEST INJURY DUE TO STAB WOUND (PNEUMOHEMOTHORAX)
Etiology: A stab wound is a specific form of penetrating trauma to the skin that results from a knife or a similar pointed object that is "deeper than it is wide. Any blunt or penetrating injury to your chest can cause lung collapse. Some injuries may happen during physical assaults or car crashes, while others may inadvertently occur during medical procedures that involve the insertion of a needle into the chest. But the most common form of pneumothorax and hemothorax, caused by open or closed chest trauma related to blunt or penetrating injuries
Excessive loss of blood
Rapid increase of pressure in chest due to compression of the vena cava with impaired venous return to the heart
Decreased blood supply to the body
Rupture of blood vessel in the thorax
Air and blood enters the pleural space
Accumulation of air and blood in the pleural space
Penetration into pleural space by an object external to the chest wall
Injury to the chest wall
Increase intrathoracic pressure and reduction in vital capacity
Decreased oxygen supply to the body
Decrease in lung expansion
Obstruction of air going into and out of the alveoli
Impaired Gas Exchange
DYSPNEA
Increase use of accessory muscles
Signs and Symptoms: Symptoms of a pneumothorax include chest pain that usually has a sudden onset. The pain is sharp and may lead to feelings of tightness in the chest. Shortness of breath, rapid heart rate, rapid breathing, cough, and fatigue are other symptoms of pneumothorax. The skin may develop a bluish color (termed cyanosis) due to decreases in blood oxygen levels. But these symptoms can be caused by a variety of health problems, and some can be life-threatening. If your chest pain is severe or breathing becomes increasingly difficult, get immediate emergency care. Physical Exam: Asses for: Absent breath sounds on affected lung Cyanosis Decreased chest expansion unilaterally Dyspnea Hypotension Sharp chest pain Subcutaneous emphysema as evidenced by crepitus on palpation Sucking sound with open chest wound Tachycardia Tachypnea Tracheal deviation to the unaffected side with tension pneumothorax
Diagnostics/ Imaging studies:
Thoracic CT: Studies show that CT is more sensitive than x-ray in detecting thoracic injuries, lung contusion, hemothorax, and pneumothorax. Early CT may influence therapeutic management. Chest x-ray: Reveals air and/or fluid accumulation in the pleural space; may show shift of mediastinal structures (heart). Chest radiography: To rule out penetration of the chest cavity Abdominal radiography in 2 views (anterior-posterior, lateral). To determine any organ affected in the abdomen Chest and abdominal ultrasonography: Focused assessment with sonography for trauma (FAST); includes 4 views (pericardial, right and left upper quadrants, pelvis) Abdominal CT scanning (including triple-contrast helical CT): Most sensitive and specific study in identifying and assessing liver or spleen injury Thoracentesis: Presence of blood/serosanguineous fluid indicates hemothorax.
Laboratory Testing: All patients with chest trauma/pneumohemothorax and possible abdominal trauma should undergo certain basic laboratory testing, especially if emergent operation is necessary:
Blood type and cross-match Complete blood count (CBC) Electrolyte levels Blood urea nitrogen (BUN) and serum creatinine level Glucose level Prothrombin time (PT)/activated partial thromboplastin time (aPTT) Venous or arterial lactate level Calcium, magnesium, and phosphate levels Arterial blood gas (ABG) Urinalysis Serum and urine toxicology screen Possible complications:
Another collapsed lung in the future Shock Hypoxemia Respiratory failure and Cardiac arrest
Nursing Management: Assess and monitor for:
Airway, breathing, circulation (ABCs) Signs of tachycardia, dyspnea, hypotension, etc. Vital signs, including the pulseoximetre I and O Level of consciousness to detect neurologic deficits Location(s) of the wound(s): Inspect all body surfaces, and document all penetrating wounds Type of penetrating weapon or object Amount of blood loss Apply a dressing over an open chest wound. ister oxygen as prescribed. Position the client in high fowler’s position. Prepare for chest tube placement until the lung has expanded fully. Monitor chest tube drainage system. Monitor for subcutaneous emphysema. Medical Management:
The priority is to maintain airway, breathing, and circulation. The most important interventions focus on reinflating the lung by evacuating the pleural air. Patients with a primary spontaneous pneumothorax that is small with minimal symptoms may have spontaneous sealing and lung re-expansion. For patients with jeopardized gas exchange, chest tube insertion may be necessary to achieve lung reexpansion. Maintain a closed chest drainage system; be sure to tape all connections, and secure the tube carefully at the insertion site with adhesive bandages. Regulate suction according to the chest tube system directions; generally, suction does not exceed 20 to 25 cm H2O negative pressure. Monitor a chest tube unit for any kinks or bubbling, which could indicate an air leak, but do not clamp a chest tube without a physician’s order because clamping may lead to tension pneumothorax. Stabilize the chest tube so that it does not drag or pull against the patient or against the drainage system. Maintain aseptic technique, changing the chest tube insertion site dressing and monitoring the site for signs and symptoms of infection such as redness, swelling, warmth, and drainage. Oxygen therapy and mechanical ventilation are prescribed as needed. Surgical interventions include removing the penetrating object, exploratory thoracotomy if necessary, thoracentesis, and thoracotomy for patients with two or more episodes of spontaneous pneumothorax or patients with pneumothorax that does not resolve within 1 week. Foley catherization: to monitor fluid resuscitation Pharmacotherapy: Tube thoracostomy: to relieve hemothorax/pneumothorax Thoracentesis: procedure in used whichina the needle is inserted through the back the chest wall into the pleural The following medications may be management of patients withofchest trauma: space (a space that exists between the two lungs and the anterior chest wall) to remove fluid or air.
Analgesics (eg, morphine sulfate, fentanyl citrate) Anxiolytics (eg, lorazepam, midazolam hydrochloride) Antibiotics (eg, cefotetan, metronidazole hydrochloride, gentamicin sulfate, vancomycin hydrochloride, ampicillin sodium-sulbactam sodium) Neuromuscular blocking agents (eg, succinylcholine, vecuronium bromide) Immune enhancement (eg, tetanus toxoid adsorbed or fluid)
** No routine pharmacologic measures will treat pneumothorax, but the patient may need antibiotics, local anesthesia agents for procedures, and analgesics, depending on the extent and nature of the injury. **
Discharge Goals:
Adequate ventilation/oxygenation maintained. Complications prevented/resolved. Pain absent/controlled. Disease process/prognosis and therapy needs understood. Plan in place to meet needs after discharge.
Discharge and Home Healthcare Guidelines:
Review all follow-up appointments, which often involve chest x-rays, arterial blood gas analysis, and a physical exam. If the injury was alcohol-related, explore the patient’s drinking pattern. Refer for counseling, if necessary. Teach the patient when to notify the physician of complications (infection, an unhealed wound, and anxiety) and to report any sudden chest pain or difficulty breathing.
Predisposing factors:
Precipitating factors:
Environment where pt lives Environment where the pt works for a living Shift of work (night) Relationship with other people
Age. More common in young adults Gender. More common in males
CHEST INJURY DUE TO STAB WOUND (PNEUMOHEMOTHORAX)
Etiology: A stab wound is a specific form of penetrating trauma to the skin that results from a knife or a similar pointed object that is "deeper than it is wide. Any blunt or penetrating injury to your chest can cause lung collapse. Some injuries may happen during physical assaults or car crashes, while others may inadvertently occur during medical procedures that involve the insertion of a needle into the chest. But the most common form of pneumothorax and hemothorax, caused by open or closed chest trauma related to blunt or penetrating injuries
Excessive loss of blood
Rapid increase of pressure in chest due to compression of the vena cava with impaired venous return to the heart
Decreased blood supply to the body
Rupture of blood vessel in the thorax
Air and blood enters the pleural space
Accumulation of air and blood in the pleural space
Penetration into pleural space by an object external to the chest wall
Injury to the chest wall
Increase intrathoracic pressure and reduction in vital capacity
Decreased oxygen supply to the body
Decrease in lung expansion
Obstruction of air going into and out of the alveoli
Impaired Gas Exchange
DYSPNEA
Increase use of accessory muscles
Signs and Symptoms: Symptoms of a pneumothorax include chest pain that usually has a sudden onset. The pain is sharp and may lead to feelings of tightness in the chest. Shortness of breath, rapid heart rate, rapid breathing, cough, and fatigue are other symptoms of pneumothorax. The skin may develop a bluish color (termed cyanosis) due to decreases in blood oxygen levels. But these symptoms can be caused by a variety of health problems, and some can be life-threatening. If your chest pain is severe or breathing becomes increasingly difficult, get immediate emergency care. Physical Exam: Asses for: Absent breath sounds on affected lung Cyanosis Decreased chest expansion unilaterally Dyspnea Hypotension Sharp chest pain Subcutaneous emphysema as evidenced by crepitus on palpation Sucking sound with open chest wound Tachycardia Tachypnea Tracheal deviation to the unaffected side with tension pneumothorax
Diagnostics/ Imaging studies:
Thoracic CT: Studies show that CT is more sensitive than x-ray in detecting thoracic injuries, lung contusion, hemothorax, and pneumothorax. Early CT may influence therapeutic management. Chest x-ray: Reveals air and/or fluid accumulation in the pleural space; may show shift of mediastinal structures (heart). Chest radiography: To rule out penetration of the chest cavity Abdominal radiography in 2 views (anterior-posterior, lateral). To determine any organ affected in the abdomen Chest and abdominal ultrasonography: Focused assessment with sonography for trauma (FAST); includes 4 views (pericardial, right and left upper quadrants, pelvis) Abdominal CT scanning (including triple-contrast helical CT): Most sensitive and specific study in identifying and assessing liver or spleen injury Thoracentesis: Presence of blood/serosanguineous fluid indicates hemothorax.
Laboratory Testing: All patients with chest trauma/pneumohemothorax and possible abdominal trauma should undergo certain basic laboratory testing, especially if emergent operation is necessary:
Blood type and cross-match Complete blood count (CBC) Electrolyte levels Blood urea nitrogen (BUN) and serum creatinine level Glucose level Prothrombin time (PT)/activated partial thromboplastin time (aPTT) Venous or arterial lactate level Calcium, magnesium, and phosphate levels Arterial blood gas (ABG) Urinalysis Serum and urine toxicology screen Possible complications:
Another collapsed lung in the future Shock Hypoxemia Respiratory failure and Cardiac arrest
Nursing Management: Assess and monitor for:
Airway, breathing, circulation (ABCs) Signs of tachycardia, dyspnea, hypotension, etc. Vital signs, including the pulseoximetre I and O Level of consciousness to detect neurologic deficits Location(s) of the wound(s): Inspect all body surfaces, and document all penetrating wounds Type of penetrating weapon or object Amount of blood loss Apply a dressing over an open chest wound. ister oxygen as prescribed. Position the client in high fowler’s position. Prepare for chest tube placement until the lung has expanded fully. Monitor chest tube drainage system. Monitor for subcutaneous emphysema. Medical Management:
The priority is to maintain airway, breathing, and circulation. The most important interventions focus on reinflating the lung by evacuating the pleural air. Patients with a primary spontaneous pneumothorax that is small with minimal symptoms may have spontaneous sealing and lung re-expansion. For patients with jeopardized gas exchange, chest tube insertion may be necessary to achieve lung reexpansion. Maintain a closed chest drainage system; be sure to tape all connections, and secure the tube carefully at the insertion site with adhesive bandages. Regulate suction according to the chest tube system directions; generally, suction does not exceed 20 to 25 cm H2O negative pressure. Monitor a chest tube unit for any kinks or bubbling, which could indicate an air leak, but do not clamp a chest tube without a physician’s order because clamping may lead to tension pneumothorax. Stabilize the chest tube so that it does not drag or pull against the patient or against the drainage system. Maintain aseptic technique, changing the chest tube insertion site dressing and monitoring the site for signs and symptoms of infection such as redness, swelling, warmth, and drainage. Oxygen therapy and mechanical ventilation are prescribed as needed. Surgical interventions include removing the penetrating object, exploratory thoracotomy if necessary, thoracentesis, and thoracotomy for patients with two or more episodes of spontaneous pneumothorax or patients with pneumothorax that does not resolve within 1 week. Foley catherization: to monitor fluid resuscitation Pharmacotherapy: Tube thoracostomy: to relieve hemothorax/pneumothorax Thoracentesis: procedure in used whichina the needle is inserted through the back the chest wall into the pleural The following medications may be management of patients withofchest trauma: space (a space that exists between the two lungs and the anterior chest wall) to remove fluid or air.
Analgesics (eg, morphine sulfate, fentanyl citrate) Anxiolytics (eg, lorazepam, midazolam hydrochloride) Antibiotics (eg, cefotetan, metronidazole hydrochloride, gentamicin sulfate, vancomycin hydrochloride, ampicillin sodium-sulbactam sodium) Neuromuscular blocking agents (eg, succinylcholine, vecuronium bromide) Immune enhancement (eg, tetanus toxoid adsorbed or fluid)
** No routine pharmacologic measures will treat pneumothorax, but the patient may need antibiotics, local anesthesia agents for procedures, and analgesics, depending on the extent and nature of the injury. **
Discharge Goals:
Adequate ventilation/oxygenation maintained. Complications prevented/resolved. Pain absent/controlled. Disease process/prognosis and therapy needs understood. Plan in place to meet needs after discharge.
Discharge and Home Healthcare Guidelines:
Review all follow-up appointments, which often involve chest x-rays, arterial blood gas analysis, and a physical exam. If the injury was alcohol-related, explore the patient’s drinking pattern. Refer for counseling, if necessary. Teach the patient when to notify the physician of complications (infection, an unhealed wound, and anxiety) and to report any sudden chest pain or difficulty breathing.
Related Documents 171j1w
Stab Wound Pathophysiology 622x4n
February 2022 0
N Stab Wound 234wt
October 2019 67
Wound 5b254r
April 2022 0
Pathophysiology 61342b
November 2019 224
Chorinho Natalino Stab f5o72
April 2023 0
Pathophysiology 61342b
November 2019 193More Documents from "Jaessa Feliciano" 4o595s
Stab Wound Pathophysiology 622x4n
February 2022 0
Isoket f5r7
November 2019 16
2c82t
December 2019 174
Piano Virtual 402c3x
December 2019 178
Exempting Circumstances 493a63
December 2019 40