Cerebrovascular Accident Nursing Care Plan 2u1js
This document was ed by and they confirmed that they have the permission to share it. If you are author or own the copyright of this book, please report to us by using this report form. Report r6l17
Overview 4q3b3c
& View Cerebrovascular Accident Nursing Care Plan as PDF for free.
More details 26j3b
- Words: 907
- Pages: 4
Nursing Problems with cues
Nursing Diagnosis with Rationale
Objectives (SMART)
Nursing Interventions
Problem: Altered level of consciousness Subjective: Patient complained of dizziness before ission. Also reported weakness and numbness on left extremities 3 hours prior to ission as verbalized by patient’s son Objective: Vital signs Blood pressure: 160/100 mmHg RR: 21, CR: 62 bmp Temp: 36.8
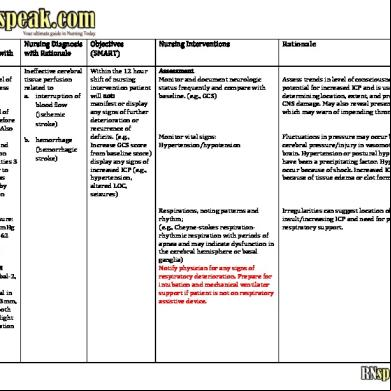
Ineffective cerebral tissue perfusion related to a. interruption of blood flow (ischemic stroke)
Within the 12 hour shift of nursing intervention patient will not: manifest or display any signs of further deterioration or recurrence of deficits. (e.g., Increase GCS score from baseline score) display any signs of increased I (e.g., hypertension, altered LOC, seizures)
Assessment Monitor and document neurologic status frequently and compare with baseline. (e.g., GCS)
GCS score: 8 Eyes-2, verbal-2, motor- 4 Pupils: equal in size: right- 3mm, left-3mm, both reactive to light accommodation
b. hemorrhage (hemorrhagic stroke)
Rationale
Assess trends in level of consciousness and potential for increased I and is useful for determining location, extent, and progression of CNS damage. May also reveal presence of TIA, which may warn of impending thrombotic CVA
Monitor vital signs: Hypertension/hypotension
Fluctuations in pressure may occur because cerebral pressure/injury in vasomotor area of the brain. Hypertension or postural hypotension may have been a precipitating factor. Hypotension may occur because of shock. Increased I may occur because of tissue edema or clot formation.
Respirations, noting patterns and rhythm; (e.g., Cheyne-stokes respirationrhythmic respiration with periods of apnea and may indicate dysfunction in the cerebral hemisphere or basal ganglia) Notify physician for any signs of respiratory deterioration. Prepare for intubation and mechanical ventilator if patient is not on respiratory assistive device.
Irregularities can suggest location of cerebral insult/increasing I and need for possible respiratory .
Diagnostic studies: CT scan: standard diagnostic study to identify location and type of stroke. May reveal ischemic infarction or hemorrhagic stroke. Usual laboratory studies for patients suspected with stroke: CBC, platelet and clotting factors like PT (INR) and PTT, ESR, fibrinogen, blood sugar
Evaluate pupils, noting size, shape, equality, light reactivity. Watch out for anisocoric pupils greater then 2mm. (e.g., Left pupil2mm, right pupil- 4mm). Notify physician immediately. It may indicate progression of hemorrhage. Prepare for further diagnostic evaluation (CT scan, laboratory studies like PT or aPTT)
Pupil reactions are regulated by the oculomotor (III) cranial nerve and are useful in determining whether the brainstem is intact. Pupil size/equality is determined by balance between parasympathetic and sympathetic enervation. Response to light reflects combined function of the optic (III) and oculomotor (III) cranial nerves.
Document changes in vision; e.g., reports of blurred vision, alterations in the visual field/depth perception. Assess higher functions, including speech, if client is alert.
Specific visual alterations reflect area of brain involved, indicate safety concerns, and influence choice of interventions. Changes in cognition and speech content are an indicator of location or degree of cerebral involvement and may indicate deterioration/increased I.
You may use stroke scale (National Institutes of Health Stroke Scale) for monitoring or evaluating progression or regression of patient’s condition. If possible obtain baseline data, as soon as patient is itted in the institution. Baseline data will serve as comparison to evaluate if management is effective or not.
(Please see discussion for further information regarding this type of assessment) Assess for nuchal rigidity, twitching, increased restlessness, irritability, onset of seizure activity,
Indicative of meningeal irritation, especially in hemorrhagic disorders. Seizures may reflect increased I/cerebral injury, requiring further evaluation and intervention.
Independent Position with head slightly elevated and in neutral position.
Reduces arterial pressure by promoting venous drainage and may improve cerebral circulation or perfusion.
Maintain bed rest, provide quiet environment, and limit visitors/activities.
Continual stimulation or activity can increase I. Absolute rest and quiet may be needed to prevent recurrence of bleeding in the case of hemorrhage.
Prevent straining at stool or holding breath. (ister laxative as prescribed, provide diapers to patient and clean under pads, provide privacy and comfort, maintain patient on complete bed rest, instruct patient not to exert effort while defecating, assist with changing of diapers)
Valsalva maneuver increases I and potentiates recurrence of bleeding.
Collaborative ister supplemental oxygen as indicated.
ister medications as indicated: Intravenous thrombolytics; tissue plasminogen activator (tPA), alteplase (Activase) This is used only for patients with ischemic stroke and not for hemorrhagic stroke.
Reduces hypoxemia, which can cause cerebral vasodilation and increase pressure/edema formation. Proven therapy for acute stroke, t-PA is useful in minimizing the size of the infarcted area by opening blocked vessels that are occluded with the clot. Treatment must be started within 3 hours of initial symptoms to improve outcomes. (please see discussion regarding t-PA medication)
(Please see discussion for more information regarding criteria of thrombolytic istration) Anticoagulants; e.g warfarin sodium (Coumadin), heparin (Enoxaparin) Antiplatelet; e.g: aspirin (ASA), clopidogrel (Plavix) Neuroprotective agents; calcium channel blockers Nomodipine (Nimotop),
Nootropics; Citicoline (Zynapse), Phenytoin (Dilantin) Prepare patient for surgery as appropriate; microvascular by or cerebral angioplasty. For patient with increased intracranial pressure, usual management is surgical evacuation or excision, ventriculostomy insertion.
May be used to improve cerebral blood flow and prevent further clotting/thrombosis is the problem. Maybe used to prevent further clotting/reduce risk of recurrence of stroke. Agents protect the brain by interrupting the destructive cascade of biochemical events to limit ischemic injury. Increases blood flow and consumption of oxygen in the brain May be used to control seizures or for sedative purposes.
Maybe necessary to resolve situation, reduce neurologic symptoms, and risk for recurrent stroke.
Nursing Diagnosis with Rationale
Objectives (SMART)
Nursing Interventions
Problem: Altered level of consciousness Subjective: Patient complained of dizziness before ission. Also reported weakness and numbness on left extremities 3 hours prior to ission as verbalized by patient’s son Objective: Vital signs Blood pressure: 160/100 mmHg RR: 21, CR: 62 bmp Temp: 36.8
Ineffective cerebral tissue perfusion related to a. interruption of blood flow (ischemic stroke)
Within the 12 hour shift of nursing intervention patient will not: manifest or display any signs of further deterioration or recurrence of deficits. (e.g., Increase GCS score from baseline score) display any signs of increased I (e.g., hypertension, altered LOC, seizures)
Assessment Monitor and document neurologic status frequently and compare with baseline. (e.g., GCS)
GCS score: 8 Eyes-2, verbal-2, motor- 4 Pupils: equal in size: right- 3mm, left-3mm, both reactive to light accommodation
b. hemorrhage (hemorrhagic stroke)
Rationale
Assess trends in level of consciousness and potential for increased I and is useful for determining location, extent, and progression of CNS damage. May also reveal presence of TIA, which may warn of impending thrombotic CVA
Monitor vital signs: Hypertension/hypotension
Fluctuations in pressure may occur because cerebral pressure/injury in vasomotor area of the brain. Hypertension or postural hypotension may have been a precipitating factor. Hypotension may occur because of shock. Increased I may occur because of tissue edema or clot formation.
Respirations, noting patterns and rhythm; (e.g., Cheyne-stokes respirationrhythmic respiration with periods of apnea and may indicate dysfunction in the cerebral hemisphere or basal ganglia) Notify physician for any signs of respiratory deterioration. Prepare for intubation and mechanical ventilator if patient is not on respiratory assistive device.
Irregularities can suggest location of cerebral insult/increasing I and need for possible respiratory .
Diagnostic studies: CT scan: standard diagnostic study to identify location and type of stroke. May reveal ischemic infarction or hemorrhagic stroke. Usual laboratory studies for patients suspected with stroke: CBC, platelet and clotting factors like PT (INR) and PTT, ESR, fibrinogen, blood sugar
Evaluate pupils, noting size, shape, equality, light reactivity. Watch out for anisocoric pupils greater then 2mm. (e.g., Left pupil2mm, right pupil- 4mm). Notify physician immediately. It may indicate progression of hemorrhage. Prepare for further diagnostic evaluation (CT scan, laboratory studies like PT or aPTT)
Pupil reactions are regulated by the oculomotor (III) cranial nerve and are useful in determining whether the brainstem is intact. Pupil size/equality is determined by balance between parasympathetic and sympathetic enervation. Response to light reflects combined function of the optic (III) and oculomotor (III) cranial nerves.
Document changes in vision; e.g., reports of blurred vision, alterations in the visual field/depth perception. Assess higher functions, including speech, if client is alert.
Specific visual alterations reflect area of brain involved, indicate safety concerns, and influence choice of interventions. Changes in cognition and speech content are an indicator of location or degree of cerebral involvement and may indicate deterioration/increased I.
You may use stroke scale (National Institutes of Health Stroke Scale) for monitoring or evaluating progression or regression of patient’s condition. If possible obtain baseline data, as soon as patient is itted in the institution. Baseline data will serve as comparison to evaluate if management is effective or not.
(Please see discussion for further information regarding this type of assessment) Assess for nuchal rigidity, twitching, increased restlessness, irritability, onset of seizure activity,
Indicative of meningeal irritation, especially in hemorrhagic disorders. Seizures may reflect increased I/cerebral injury, requiring further evaluation and intervention.
Independent Position with head slightly elevated and in neutral position.
Reduces arterial pressure by promoting venous drainage and may improve cerebral circulation or perfusion.
Maintain bed rest, provide quiet environment, and limit visitors/activities.
Continual stimulation or activity can increase I. Absolute rest and quiet may be needed to prevent recurrence of bleeding in the case of hemorrhage.
Prevent straining at stool or holding breath. (ister laxative as prescribed, provide diapers to patient and clean under pads, provide privacy and comfort, maintain patient on complete bed rest, instruct patient not to exert effort while defecating, assist with changing of diapers)
Valsalva maneuver increases I and potentiates recurrence of bleeding.
Collaborative ister supplemental oxygen as indicated.
ister medications as indicated: Intravenous thrombolytics; tissue plasminogen activator (tPA), alteplase (Activase) This is used only for patients with ischemic stroke and not for hemorrhagic stroke.
Reduces hypoxemia, which can cause cerebral vasodilation and increase pressure/edema formation. Proven therapy for acute stroke, t-PA is useful in minimizing the size of the infarcted area by opening blocked vessels that are occluded with the clot. Treatment must be started within 3 hours of initial symptoms to improve outcomes. (please see discussion regarding t-PA medication)
(Please see discussion for more information regarding criteria of thrombolytic istration) Anticoagulants; e.g warfarin sodium (Coumadin), heparin (Enoxaparin) Antiplatelet; e.g: aspirin (ASA), clopidogrel (Plavix) Neuroprotective agents; calcium channel blockers Nomodipine (Nimotop),
Nootropics; Citicoline (Zynapse), Phenytoin (Dilantin) Prepare patient for surgery as appropriate; microvascular by or cerebral angioplasty. For patient with increased intracranial pressure, usual management is surgical evacuation or excision, ventriculostomy insertion.
May be used to improve cerebral blood flow and prevent further clotting/thrombosis is the problem. Maybe used to prevent further clotting/reduce risk of recurrence of stroke. Agents protect the brain by interrupting the destructive cascade of biochemical events to limit ischemic injury. Increases blood flow and consumption of oxygen in the brain May be used to control seizures or for sedative purposes.
Maybe necessary to resolve situation, reduce neurologic symptoms, and risk for recurrent stroke.
Related Documents 171j1w
Cerebrovascular Accident Nursing Care Plan 2u1js
October 2019 321
Nursingcrib.com Nursing Care Plan Cerebrovascular Accident (cva) 3y6367
December 2019 454
14 Cerebrovascular Accident Nursing Care Plans 6v6w28
December 2019 138
Pathophysiology Of Cerebrovascular Accident 49a3
November 2020 0
Cerebrovascular Accident Ppt 6n2p6p
December 2019 70
Case Study Cerebrovascular Accident 2b39q
December 2019 69More Documents from "Cyrus De Asis" 4ye6h

Nursing Care Plan Of Pressure Ulcers 2b4b8
October 2019 70
Acute Glomerulonephritis _agn_ Nursing Care Plan 204q5a
November 2019 319
Pathophysiology Of Diabetes 3i4o5i
November 2019 89
Congestive Heart Failure Schematic Diagram 266u22
October 2021 0
Cerebrovascular Accident Nursing Care Plan 2u1js
October 2019 321