Sample Filled Up - Dole Employer's Work Accident Report 5w331d
This document was ed by and they confirmed that they have the permission to share it. If you are author or own the copyright of this book, please report to us by using this report form. Report r6l17
Overview 4q3b3c
& View Sample Filled Up - Dole Employer's Work Accident Report as PDF for free.
More details 26j3b
- Words: 591
- Pages: 1
DOLE/BWC/OHSD/IP-6 Republic of the Philippines DEPARTMENT OF LABOR AND EMPLOYMENT Region I EMPLOYER’S WORK ACCIDENT/ILLNESS REPORT (This report shall be submitted by the employer for every accident or illness to the Regional Office having jurisdiction on or before the 20th day of the month following the date of occurrence.)
EMPLOYER
INJURED OR ILL PERSON Occupational History
ACCIDENT OR ILLNESS
NATURE & EXTENT OF INJURY OR ILLNESS CAUSE OF ACCIDENT OR ILLNESS
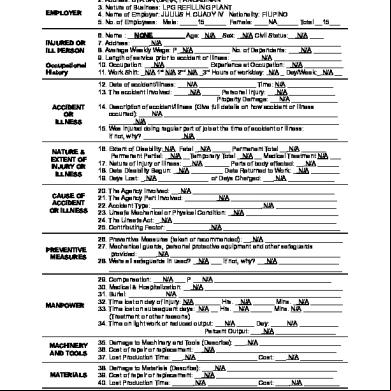
1. Establishment: ORO OXYGEN CORPORATION 2. Address: STA.BARBARA, PANGASINAN 3. Nature of Business: LPG REFILLING PLANT 4. Name of Employer: JULIUS H. CUADY IV Nationality: FILIPINO 5. No. of Employees: Male: _____15______ Female: ____NA______ Total __15___ 6. Name : __NONE_________ Age: _N/A__Sex: _ N/A Civil Status:__ N/A ____ 7. Address: _____ N/A __________________________________________________ 8. Average Weekly Wage: P_ N/A __________ No. of Dependents: ___ N/A ________ 9. Length of service prior to accident or illness: ________ N/A ___________________ 10. Occupation: __ N/A ____________ Experience at Occupation: _ N/A ___________ 11. Work Shift: _N/A 1st N/A 2nd N/A _3rd Hours of work/day: N/A _ Day/Week:_ N/A __ 12. Date of accident/illness: __ N/A ________________ Time: N/A _____________ 13. The accident involved: ____ N/A _____ Personal Injury: __ N/A _____________ Property Damage: __ N/A _____________ 14. Description of accident/illness (Give full details on how accident or illness occurred): ___ N/A _________________________________________________ _______ N/A ______________________________________________________ 15. Was injured doing regular part of job at the time of accident or illness: If not, why? ___________ N/A ________________________________________ 16. Extent of Disability: N/A Fatal _ N/A _____ Permanent Total __ N/A _______ Permanent Partial: _ N/A __Temporary Total _ N/A __ Medical Treatment N/A ___ 17. Nature of Injury or Illness: __ N/A _______ Parts of body affected: __ N/A ______ 18. Date Disability Begun: _ N/A _________ Date Returned to Work: _ N/A ________ 19. Days Lost: _ N/A ______________ or Days Charged: ___ N/A _____________ 20. The Agency Involved: __ N/A ________________________________________ 21. The Agency Part Involved: _________ N/A ______________________________ 22. Accident Type: _______________________________ N/A _________________ 23. Unsafe Mechanical or Physical Condition: _ N/A __________________________ 24. The Unsafe Act: _ N/A ______________________________________________ 25. Contributing Factor: ____________ N/A _________________________________
PREVENTIVE MEASURES
26. Preventive Measures (taken or recommended): __ N/A ______________________ 27. Mechanical guards, personal protective equipment and other safeguards provided: _____ N/A ________________________________________________ 28. Were all safeguards in used? _ N/A ___ If not, why? __ N/A _________________ __________________________________________________________________
MANPOWER
29. Compensation: __ N/A ___ P __ N/A _________________________________ 30. Medical & Hospitalization: __ N/A _______________________________________ 31. Burial: __________ N/A ______________________________________________ 32. Time lost on day of injury: N/A _______ Hrs. _ N/A ______ Mins. _ N/A _________ 33. Time lost on subsequent days: N/A __ Hrs. _ N/A ______ Mins. N/A ___________ (Treatment or other reasons) 34. Time on light work or reduced output: __ N/A _____ Day: ____ N/A ___________ Percent Output: ___ N/A _________________
MACHINERY AND TOOLS
35. Damage to Machinery and Tools (Describe): ___ N/A _______________________ 36. Cost of repair or replacement: __ N/A __________________________________ 37. Lost Production Time: ___ N/A _________________ Cost: ___ N/A ____________
MATERIALS
38. Damage to Materials (Describe): ___ N/A _______________________________ 39. Cost of repair or replacement: __ N/A _________________________________ 40. Lost Production Time: ______ N/A ______________ Cost: ____ N/A __________
EQUIPMENT
41. Damage to Equipment (Describe): __ N/A ________________________________ 42. Cost of repair or replacement: ______ N/A ________________________________ 43. Lost production time: _________ N/A ____________________________________
I HEREBY CERTIFY on my honor to the accuracy of the foregoing information: JANUARY 8, 2019 Date MARK ARTEM APALLA_/ Plant Supervisor Investigating Officer & Position
PETER M. CAUSIN POM/Employer
EMPLOYER
INJURED OR ILL PERSON Occupational History
ACCIDENT OR ILLNESS
NATURE & EXTENT OF INJURY OR ILLNESS CAUSE OF ACCIDENT OR ILLNESS
1. Establishment: ORO OXYGEN CORPORATION 2. Address: STA.BARBARA, PANGASINAN 3. Nature of Business: LPG REFILLING PLANT 4. Name of Employer: JULIUS H. CUADY IV Nationality: FILIPINO 5. No. of Employees: Male: _____15______ Female: ____NA______ Total __15___ 6. Name : __NONE_________ Age: _N/A__Sex: _ N/A Civil Status:__ N/A ____ 7. Address: _____ N/A __________________________________________________ 8. Average Weekly Wage: P_ N/A __________ No. of Dependents: ___ N/A ________ 9. Length of service prior to accident or illness: ________ N/A ___________________ 10. Occupation: __ N/A ____________ Experience at Occupation: _ N/A ___________ 11. Work Shift: _N/A 1st N/A 2nd N/A _3rd Hours of work/day: N/A _ Day/Week:_ N/A __ 12. Date of accident/illness: __ N/A ________________ Time: N/A _____________ 13. The accident involved: ____ N/A _____ Personal Injury: __ N/A _____________ Property Damage: __ N/A _____________ 14. Description of accident/illness (Give full details on how accident or illness occurred): ___ N/A _________________________________________________ _______ N/A ______________________________________________________ 15. Was injured doing regular part of job at the time of accident or illness: If not, why? ___________ N/A ________________________________________ 16. Extent of Disability: N/A Fatal _ N/A _____ Permanent Total __ N/A _______ Permanent Partial: _ N/A __Temporary Total _ N/A __ Medical Treatment N/A ___ 17. Nature of Injury or Illness: __ N/A _______ Parts of body affected: __ N/A ______ 18. Date Disability Begun: _ N/A _________ Date Returned to Work: _ N/A ________ 19. Days Lost: _ N/A ______________ or Days Charged: ___ N/A _____________ 20. The Agency Involved: __ N/A ________________________________________ 21. The Agency Part Involved: _________ N/A ______________________________ 22. Accident Type: _______________________________ N/A _________________ 23. Unsafe Mechanical or Physical Condition: _ N/A __________________________ 24. The Unsafe Act: _ N/A ______________________________________________ 25. Contributing Factor: ____________ N/A _________________________________
PREVENTIVE MEASURES
26. Preventive Measures (taken or recommended): __ N/A ______________________ 27. Mechanical guards, personal protective equipment and other safeguards provided: _____ N/A ________________________________________________ 28. Were all safeguards in used? _ N/A ___ If not, why? __ N/A _________________ __________________________________________________________________
MANPOWER
29. Compensation: __ N/A ___ P __ N/A _________________________________ 30. Medical & Hospitalization: __ N/A _______________________________________ 31. Burial: __________ N/A ______________________________________________ 32. Time lost on day of injury: N/A _______ Hrs. _ N/A ______ Mins. _ N/A _________ 33. Time lost on subsequent days: N/A __ Hrs. _ N/A ______ Mins. N/A ___________ (Treatment or other reasons) 34. Time on light work or reduced output: __ N/A _____ Day: ____ N/A ___________ Percent Output: ___ N/A _________________
MACHINERY AND TOOLS
35. Damage to Machinery and Tools (Describe): ___ N/A _______________________ 36. Cost of repair or replacement: __ N/A __________________________________ 37. Lost Production Time: ___ N/A _________________ Cost: ___ N/A ____________
MATERIALS
38. Damage to Materials (Describe): ___ N/A _______________________________ 39. Cost of repair or replacement: __ N/A _________________________________ 40. Lost Production Time: ______ N/A ______________ Cost: ____ N/A __________
EQUIPMENT
41. Damage to Equipment (Describe): __ N/A ________________________________ 42. Cost of repair or replacement: ______ N/A ________________________________ 43. Lost production time: _________ N/A ____________________________________
I HEREBY CERTIFY on my honor to the accuracy of the foregoing information: JANUARY 8, 2019 Date MARK ARTEM APALLA_/ Plant Supervisor Investigating Officer & Position
PETER M. CAUSIN POM/Employer
Related Documents 171j1w
Sample Filled Up - Dole Employer's Work Accident Report 5w331d
November 2021 0
Denr Qtrly Report Form-filled Up 4thqtr10 601z47
May 2020 9
Discharge Permit Application Form Sample Filled Up dz3g
January 2022 0
Sample Omr Sheet Filled 6u434k
December 2019 70
Pf Closure Forms - Sample Filled 3yg43
December 2019 57